1.8 million. That’s a little more than the population of Phoenix, the fifth most populous city in the United States. 1.8 million. That’s a little less than the number of people diagnosed with cancer each year. 1.8 million is also the number of individuals held in American correctional institutions at any given time in 2024. In addition to the individuals currently incarcerated, the United States releases over 7 million people from jail and more than 600,000 people from prison each year. The transition from incarceration back into the community constitutes a vulnerable time for the individuals facing this change.
To support these transitions in care for people leaving incarceration, the Health Resources Services Administration (HRSA) announced last year nearly $52 million in awards to “increase access to high-quality primary care for people soon to be released from incarceration and reentering the community.” This funding will allow 54 HRSA-funded health centers, to implement “innovative approaches” to support individuals during the 90 days prior to their release. With the grant, health centers can focus on ensuring a smooth transition of care, with emphasis on access to primary care, including mental health and substance use services. With as many as 80% of returning community members having a chronic medical, psychiatric, and or substance use disorder, this grant highlights the need for supportive services to facilitate reentry.
For practices without specific grant funding, supporting transitions back to the community remains a vital part in both individual health outcomes and for the strength of the healthcare system. Almost half of all incarcerated people are in rural jails and prisons. With funding cuts to Medicaid from the “One Big Beautiful Bill Act,” many rural hospitals will be forced to cut back on operations or close entirely. Community and rural health centers will play an increasingly large role in supporting these individuals. This emphasizes the need for rural hospitals, health centers, and community-based organizations to work together.
Azara’s comprehensive population health management solutions enable organizations to care for the individual and support the population by tracking currently incarcerated or recently released populations, managing medical and behavioral health needs, and identifying social care needs.
Tracking Individuals Prior to Release
To streamline tracking and support for individuals currently incarcerated from the general patient population, practices can create custom cohorts to identify this population within DRVS.

Once added to a cohort, practices can identify patients at the point of care by leveraging the Patient Visit Planning report (PVP) and throughout DRVS using the cohort filter. The cohort can be leveraged to identify patients who require screenings for social risk factors or those who may be eligible for Medicaid or enrollment into a health home.
A cohort of individuals during the 90 days prior to release also facilitates the support of these patients within Azara Care Connect (ACC).
Providing Wrap-Around Care Prior to Release
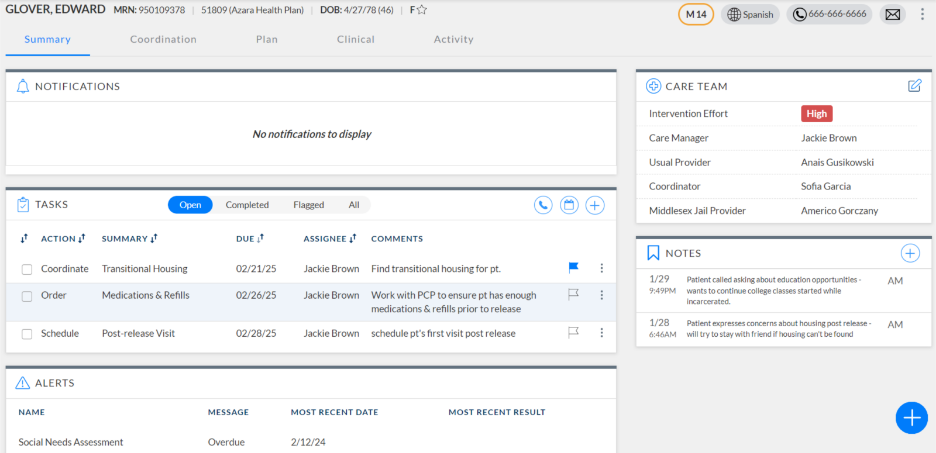
ACC provides an integrated solution to efficiently manage and coordinate care for individuals prior to their return to the community. Within ACC, Care Managers can document and track activities related to pre-release activities, such as coordinating medications post-release, scheduling follow-up visits, and screening for social care needs.
Data Insights at the Point of Care
Before seeing a patient experiencing incarceration, providers, nurses, and other care team members can generate the PVP report to identify screening opportunities for patients on the schedule. With a high rate of chronic medical and behavioral health conditions experienced by justice-involved populations, timely screening is critical for providing needed and appropriate services. Alerts such as Hemoglobin A1c, Substance Use Screening, and Suicide Risk Assessment can help identify the medical needs of the individual post-incarceration.
For practices with the Controlled Substance module, providers can easily identify patients with an opioid use disorder diagnosis who do not have a Narcan prescription. For practices with the HIV and Hep C modules, care teams be alerted to screen populations for a potential diagnosis and provide appropriate care, such as immunizations and viral load testing.
Supporting Population Health Needs
For needs at the population level, organizations can turn to custom registries and care effectiveness reports to manage key populations. Registries related to chronic medical conditions such as diabetes, hypertension, and asthma provide insights into patients’ current clinical complexity, medication needs, and comorbidities. For patients at risk of HIV, practices can understand PrEP prescriptions and HIV screening results.
With care effectiveness reports, practices can easily track changes in chronic disease control, from A1c and blood pressure, to PHQ-9 and GAD-7 scores.
Conclusion
Population health platforms like Azara DRVS and Azara Care Connect play a crucial role in supporting the transitions of incarcerated individuals back into the community. By enabling care teams to proactively identify health needs, coordinate essential services, and monitor care effectiveness, these solutions help bridge gaps in care and ensure continuity for a vulnerable population. Ultimately, leveraging data-driven insights and timely interventions foster improved health outcomes, reduce recidivism, and empower practices to support individuals with comprehensive, wrap-around care during this critical transition period.
Related Articles

Why Community Trust Is the Foundation of Population Health
Explore Insights
From Delays to Action: How Real-Time Data Transforms Transitions of Care
Explore Insights